so I'm just going to go over a little bit of just basically what prion disease
is what a prion is. So a prion stands for a protein that's infectious most
infectious organisms have DNA or RNA-- what we call nucleic acids-- and prions
are unusual in that they are transmissible but they don't have any
DNA and RNA so they're kind of a group all into themselves and they're not
degradable by typical sterilization so in order to sterilize you have to use
specific procedures and the way prion disease work is that we all have normal
prion proteins that's the yellow PrPc that we have in our body most of it's in
our brain some of it's in our stomach we don't know exactly what it does but it
probably has some housekeeping function in the brain and we all have that and
then for whatever reason we come across and infectious prpsc which stands for
scrapie protein that's the prion protein that causes the disease comes in contact
with the normal prion protein and then it converts the normal prion protein
into itself in kind of this auto catalytic cycle so in order to have
prion disease you need to have PRPC or normal prion
proteins--and this is important specifically for Dr Collinge's talk
tomorrow, when he talks about his treatment study and the importance of
blocking PRPC. so just keep that in mind once you have the abnormal prion
proteins they tend to aggregate and form seeds and then they cause things like
oligomers and fibrils and you get this kind of exponential curve that you see
where you get rapid spreading so that's what happens at the molecular level. if
you look at the brain tissue you can look at it in a variety of ways one of
the ways it's called H&E staining where the brain develops these holes or
vacuoles which gave it its original terminology of a spongiform
encephalopathy because the brain resembles spongy tissue then you can
also do immunohistochemistry and take an antibody
that binds to the abnormal prion protein and stain for that and that's what
those brown deposits are in the right hand slide is the abnormal prion protein
itself so when someone goes for autopsy at the surveillance Center both of these
are done and that's how we screen for prion disease and brains so animals also
have prion diseases and sheep and goat they have a prion disease called scrapie
which came about because one of the symptoms that sheep and goat get is they
get this itching and it causes them to scratch up against surfaces and then
cows get something called bovine spongiform encephalopathy what is
sometimes referred to as mad cow disease and then in the u.s. we have something
called chronic wasting disease which is a very unusual prion disease that affect
deer elk moose and caribou and at the end of the talk I'm going to talk
specifically about CWD and why we care about it specifically as family members
and also scientifically especially in the US. so if you look at the
epidemiology or the occurrence of CJD in the american population actually
across the world the one statistic that's usually thrown out is the one per
million statistic and this is something called an incidence and what it means is
that there's one new case per million individuals per year across the entire
population but as we'll learn later not everyone gets CJD in fact it's usually a
mid to late life illness and some people live longer than a year so that
statistic whereas it's important for public health because that's how you
look at incidences of the disease psychologically it makes it sound like
it's much rarer than perhaps what it is. so perhaps a better way of framing how
common the disease is is to look at how many deaths per year occur in the u.s.
due to prion disease or CJD and if you look at that statistics it's about one
in every six the one in every 10,000 US us deaths are due to prion disease so
that's not a common disease but it certainly is maybe not as rare
that one-in-a-million number may initially make you think so when you go
to your legislators on Monday I would advocate that you use the one in 10,000
deaths per year of CJD as opposed to the incidence members of one in a million
because most people are going to realize what incidence is so to take an example
of Ohio we have about ten and a half million people so if you look at the
incidence we would expect about ten and a half new cases per year as we'll talk
about later about 25 percent of cases lived longer than a year so you would
have about two and a half cases carried over from the year before. so if you look
at kind of a low estimate it wouldn't be unusual and actually be expected to have
13 active cases in Ohio alone at any given time. so again this is not a common
disease but I think it's a much more common than people might think again
from that one-in-a-million number. if you looked at the causes of prion disease,
most people especially in the medical community and in the media know it to be
an acquired illness mostly from the BSE epidemic or mad cow epidemic but in fact
the vast majority of human prion diseases are due to sporadic illness and
what we mean by sporadic illnesses we think what happens is the normal prion
protein sometimes undergoes of spontaneous Misfolding on its own and
converts them to the abnormal prion protein and starts that Auto catalytic cycle
that we talked about in the first couple of slides but it's not acquired from an
infection that we know if it's not genetic it seems to happen on its own
accord so that's about 85% of cases. about 10 to 15% are due to what we call
genetic etiologies and that could be genetic CJD, fatal familial insomnia or
GSS and I'll talk specifically about what those different genetic prion
diseases are later and then by far the least common cause of prion disease are
the acquired forms and that's well under 1% and that includes things like kuru
iatrogenic CJD and variant CJD which we'll talk about
later so if you look at the age of onset of the disease it tends to be a disease
of middle to late life but if you break it down by etiology you do see certain
peaks and that is variant CJD in general tends to occur and much younger people
so people in their teens 20s and 30s genetic CJD tends to occur more in
midlife like 50s and 60s and then sporadic CJD tends to be more of a later
life illness with a mean age of onset of about 62 but it's important to remember
that there's a lot of variation in between so for example we've seen
sporadic CJD and people as young as 13 or 14 and we've seen variant CJD and
people as old as 50 so you know this is just a generalization there's a lot of
variability within it the oldest in the US was 98 sporadic yeah so if you look
at how long people survive with prion disease as you well unfortunately all
know it's a very quick illness. the vast majority of people pass within one year
but there are some cases that live longer than a year about a quarter some
of them can live to three years but again that's unusual
the vast majority will pass away within four to six months of the symptoms
starting and many of you are well aware of the symptoms of CJD
what you may not be well aware of is that CJD can present in a variety of
different ways so in fact people very rarely present with what we would call
the classic CJD presentation which would be cognitive
problems or dementia problems walking and steadiness and the myoclonus or the
jerking movements that's only going to be a presentation in a very small subset
of people a lot of people will just present with cognitive problems so they
may be misdiagnosed as having Alzheimer's disease or another form of
dementia some may affect with very sudden visual changes and may be
misdiagnosed as having stroke some may just present with what we call
ataxia or an unsteady gait and be misdiagnosed as something else so in
general the rule that I have is there's no rule in how a CJD can present we
certainly seen a variety of different presentations but at least as time goes
on they tend to look very similar but of course you don't have that luxury in the
beginning of the illness. so diagnosing CJD it's a clinical diagnosis in life
the only way to definitively diagnose it is by looking at the brain tissue
preferably at autopsy and we do this by looking at the clinical symptoms so
most patients will have dementia many will have myoclonus or that's the
twitches that we talked about They'll have cerebellar or visual symptoms so
cerebellar symptoms are unsteady gait almost like a drunken walking or they
may have incoordination and visual symptoms can be a variety of things like
visual hallucinations or it could be a depth misperception they can have
weakness and tremors and sometimes even have parkinson's-like symptoms of kind
of a shuffling gait and then at the very end of the disease people reach a state
of what's called akinetic mutism which is a lack of voluntary speech and
movement unfortunately rather not specific as you see this in most end
stages of dementia but you typically do see this in most
cases of CJD towards the end and then we use a variety of different diagnostic
tests but we'll go about in detail after this one of them is called the
electroencephalogram or EEG which looks at brain waves and there's a finding
called periodic sharp wave complexes that can be suggestive of CJD and I'll
show you an example of that and then there's a variety of different spinal
fluid tests that can be done the who classification World Health Organization
classification only includes one of them currently called 1433 but a variety of
other different spinal fluid tests are also now used and
we'll talk about them and then the brain MRI also can be suggestive of CJD
by having different abnormalities in different areas of the brain on a very
specific sequence called diffusion-weighted imaging and I'll show
you an example of that as well so this is an example of periodic sharp wave
complexes on the EEG. EEGs --I agree with Richard we were talking about this at
the last session-- become kind of unhelpful in the diagnosis of CJD
currently but it is important to rule out other things like seizures so we
still use that. this is an example of a brain MRI of a patient with sporadic CJD
the specific sequences that we like to look at is called diffusion weighted
imaging and that's done on most MRIs nowadays and we look at two specific
areas and CJD one is the basal ganglia or the middle part of the brain and that
tends to show brightness or it could be the outside part of the brain called the
cortex in kind of this cortical ribboning pattern and this can be quite
suggestive of CJD in the appropriate clinical context meaning that the
patient looks like they have symptoms of CJD
and other things have been ruled out I think in some cases the brain MRI is
sometimes then the first initial suggestion of CJD so one case that we
had many years ago was a case from DC that presented to us four suspected CJD
and I examined him and he was pretty normal he had a normal memory testing
his exam was normal and then we looked at his MRI and this is actually his MRI
his only complaint was he used to do yoga and he could only do head stands
for two minutes every morning whereas before he could do it
five minutes and the only reason he had gotten an MRI was because he had been in
a bike race and he fell off and hit his head and the neurologists ordered a
brain scan and this is what happened so of course this is a case of someone who
had an MRI that looked like prion disease and a patient who did not look
like to add prion disease and this was how the suspicions arose
and then we followed the patient over time and they they did develop prion
disease and past two months later so in certain circumstances I think this has
led to an earlier diagnosis in some cases when clinicians may not have
suspected the disease so in that regard I think it's been helpful and then there
are a variety of different spinal fluid test there's two spinal fluid test that
we use that are kind of just markers of brain cell damage and that's 1433 which
at the surveillance Center is generally reported as positive negative or
ambiguous and then we have the total tau protein which is reported as a number so
you could have a tau protein level of one or it could be in the tens of
thousands and in general the higher the number sometimes the more suggestive of
CJD it can be in the right patient but these are only markers of brain cell
damage so they can be elevated in other conditions so for example people that
have seizures at mass brain tumors head injury they can all have elevated
markers of brain cell damage so it's not very specific for prion disease itself
and then we recently started using a very disease specific test called
real-time quaking induced conversion otherwise known as RT- QuIC which
actually detects the abnormal prion protein itself so it's kind of the first
disease specific marker that we have and you're going to hear a lot about that in
the conference this weekend and people doing this test on a variety of
different tissues so doctor Zanusso will talk about using it on nasal epithelium
Dr. Zhu will talk about using it on skin so it will pop up a lot and it's
very specific for the disease itself because it looks at the abnormal protein
the way it works is they take a plate with normal prion proteins in it and
then they take a sample that presumably has abnormal prion protein in it and
then they label it with what's called Thioflavin T and put it for lack of
a better term a shake and bake oven --sorry dr. Rhodes that I just described
as that -- but and what will happen is it kind of
exploits that prion paradigm where it converts normal prion proteins into
abnormal prion proteins and you start getting aggregation of these proteins
that the star fluorescent binds to and then you can see that and that's a
positive test that lets you know that there's presence of abnormal prion
proteins in there. now, the reason why it's rather specific is we would not
expect to see any abnormal prion proteins and any other condition so
that's its power and then when we talk about different diagnostic tests we
often talk about things like sensitivity and specificity. Sensitivity is how
good a test is at detecting a specific disease and generally and that's not a
specific problem in our field because we have a lot of tests that have relatively
high sensitivity. it's the specificity that until fairly recently has been a
problem and specificity is how sure you are that the disease you're trying to
detect is the actual disease that you're trying to detect. so in RT-QuIC the
sensitivity is high at 95% and relatively almost 100% specific for the
disease because we wouldn't expect it in anything else I'm going to talk a
little bit about the difference between the surveillance Center and the Mayo
Clinic because I know some families have had specimens sent to both and the
different results so the tests are done differently from a lab standpoint and
also when you send the specimen to the Mayo Clinic the physician has to
actually order specific tests they have to know to order 14-3-3 and if they want
tau they have to know to order that a lot of clinicians may not know that tau
could be helpful in their diagnosis so it's not ordered RT quic is also only
available at the prion surveillance center so if that went to Mayo you're
not going to get the RT quic. one of the benefits of receiving spinal fluid at
the surveillance center is in essence patients or clinicians don't really need to
know what they're ordering they just need to know that there's a suspicion of
prion disease and then we automatically do all three tests so
that can be helpful for the clinicians the other helpful thing is that if we
have a positive test then we have people that will contact the clinician saying
that we have this autopsy program that I believe you're going to hear about in
detail on Sunday that's funded through the CDC. I just wanted to end a little
bit on sporadic CJD talking about sporadic CJD molecular subtypes because
you'll hear about this and it's very confusing. so sporadic CJD has different
molecular subtypes that behave in different manners and the reason why we
care about that is because it looks differently on the brain tissue
it may look differently clinically and also the diagnostic tests may be
different and generally you'll hear these terms turn around like mm 1 mm 2
VV 2 and what that refers to is those first two letters are what's called a
polymorphism at a specific part of the prion protein gene that's kind of like a
flavor that we all have so we all can have one of three flavors we could have
mm mV or VV and these sometimes dictate the course of the disease
and what they look like clinically and Neuropathologically so we take those two
letters and we also match it with the prion protein type that's usually
detected off a Western blot and that's where you get the number from so for
example a patient who has mm polymorphism at codon 129 and a prion
protein of type 1 would be mm 1 so just so you hear these you know alphabet soup
going around that's what that refers to
so we talked a little bit about genetic prion disease the way genetic prion
disease works is we all have a normal prion protein gene that makes normal
prion proteins but in some individuals there can be a mutation in that gene
that instead of allowing them to make normal prion protein it allows them to
make a mutated form of the prion protein that has a much
higher chance of converting to the abnormal prion protein and then causing genetic
prion disease so when people have genetic prion disease their blood
relatives have a 50/50 chance of also inheriting the mutation but the
likelihood of them developing the illness is something called penetrance
so not everyone who has a mutation will develop the disease there are some
people who will not and penetrance means that it's the likelihood that you'll
become ill with CJD if you have the mutation and this is from a very
important paper that Eric Minkel and a lot of other colleagues put together
looking at different penetrance rates in different mutations and what you can see
is at the top of the table those are mutations that have very low
penetrance so you know they have you know maybe a 1% 5% chance of developing
the disease if they had the mutation that's important to know if you're a
family member who's deciding or whether or not you want to be tested because you
want to know what your risk is as you would expect the right-hand column where
there's red bars are reflects the percentage of people that had a positive
family history and if you have a mutation that has low penetrance
logically you're not going to have a lot of other family members that have become
ill there are many mutations unfortunately in prion disease though
towards the bottom those like E200k or P102L where the penetrance is quite
high and generally is associated with aged nearing a hundred percent but it's
not the same penetrance level for every mutation so if you belong to a genetic
family it's very important to know what the mutation is because that's going to
reflect the likelihood of developing illness if you have it so you want to
make sure that you'll have that you have that information so I talked about three
different genetic prion diseases. genetic CJD is kind of easy because it's called
that because it resembles sporadic CJD the most common mutation of genetic CJD
is the e200K mutation and a lot of the clinical symptoms and
diagnostic tests that we use for sporadic CJD are also positive in
genetic CJD although not always there's another genetic prion disease called
fatal familial insomnia which is due to a very specific mutation as the name
denotes insomnia tends to be a prominent symptom but you can also have very
prominent neuropsychiatric symptoms of anxiety and hallucinations and patients
with FFI you do develop cognitive issues they usually very late in the illness so
this is a genetic prion disease that sometimes doesn't really resemble what
we classically think of as CJD similarly Gerstmann-Straussler- Sheinker
syndrome or GSS is due to several different mutations
it also looks very unlike most cases of sporadic CJD mainly because the illness
duration is much longer so most patients with GSS can live about five years
sometimes up to ten years and they typically either have a very early
cerebellar presentation meaning that they have incoordination or problems
walking or they may have an initial parkinson's-like presentation where they
have a shuffling slow gait and then they typically don't develop other symptoms
characteristic of prion disease until much later in the illness. so this is a
genetic prion disease that if you don't know that you have it in your family
often will go undiagnosed until someone has considered it a possibility in that
family and with FFI and GSS a lot of the diagnostic tests that we use like CSF
tests brain MRI they're often negative in these tests that also leads to
difficulty in diagnosing these conditions. Moving on to acquired prion
disease most people know the story of kuru it's happened in a tribe in Papua
New Guinea where they partook in cannibalism as part of their death
rituals basically probably what happened is one individual developed
CJD. the loved ones consumed brain tissue and then continued to pass from
generation to generation so once cannibalism was ruled out the incidence
of kuru drastically reduced and I don't think they have had any case of kuru in
some time now but kuru is important because it really is what kind of
suggested that prion disease may be transmissible and that led to the
discovery of something called iatrogenic CJD. So Iatrogenic means medically
induced so these are cases of CJD that are transmitted through very specific
medical procedures and these are things like corneal transplants or
neurosurgical instrumentation but most commonly due to material taken from
cadavers. for example human growth hormone used to be taken from cadavers
to treat patients with a short stature we don't do that anymore because we know
the risk of prion disease and fortunately we can also synthesize human
growth hormone in the lab so we don't have to do that anymore also . there's a
covering of the brain called the dura mater that used to be taken from
cadavers to cover holes and neuro surgeries and that also is no longer
done because we can create that synthetically but we learned a lot from
iatrogenic CJD in that sometimes the time from the exposure to the infection
to the time that patients became he'll can be quite extended sometimes up to
decades and just a general rule of thumb for acquired prion disease with one very
specific exception is that in order to transmit prion disease prion material
has to be taken essentially from the central nervous system and then it has
to be introduced in another patient central nervous system injected into the
body or and ingested in large quantities in order to transmit them the disease
the one exception for this is variant CJD because we do know that variant CJD
is a little different and that it resides outside of the CNS specifically
and things like the spleen tonsils and appendix
and can actually be transmitted through blood but at least epidemiologically
there's only evidence that variant CJD can be transmitted in that fashion
so variant CJD is CJD in humans that due to eating meat contaminated with bovine
spongiform encephalopathy or mad cow disease it tends to be a young disease
so onsets typically in 20s or the 30s and it has a little longer duration than
classical sporadic CJD often over a year and their initial clinical presentation
is a little different and that they tend to have more psychiatric symptoms and
sensory symptoms at the beginning of their presentation often times 14-3-3 and
EEGS are negative and they can have different brain MRI findings from what
we typically see in sporadic CJD something called the pulvinar sign or
hockey-stick sign that's somewhat specific for variant as opposed to
sporadic CJD and then at least only in variant CJD you can also do a tonsil
biopsy to detect the abnormal prion protein that causes variant CJD but this
is the only type of prion disease where you could do that because it's unique in
that mechanism that it resides outside the central nervous system so if you
look at the cases of variant CJD worldwide the mad cow epidemic happened
in the UK so the majority of cases a variant CJD have occurred in the UK and
then most others were in European countries we've had four cases in the US
but all of them were thought to be acquired overseas and I think probably
Ryan Maddox from the CDC will talk a little bit more in detail about that on
Sunday today we have a total of about 231 cases which is quite remarkable
because quite a number of people were exposed to meat contaminated with BSE
that have such a low numbers is fairly fortunate if you look at the death rates
of variant CJD in the UK over time the BSE epidemic happened in 1980s
then the peak death rate in the UK occurred about the year 2000 which leads
us to believe that the mean incubation period so time from exposure to BSE to
becoming ill is about 10 years and we've seen a very steady tail of cases after
that but clearly the diseases and the decline and I don't think there's anyone
currently alive with respect to variant CJD --am i correct?-- so that's good and
haven't been for about a year now right. there is another sticky point however
with variant CJD and that is although only 231 cases have occurred to date a
lot of people were exposed to BSE so the concern is are there asymptomatic
carriers of the infection who they themselves may or may not become ill but
also may or may not be transmissible to other people via things like blood
transfusion so the UK did a study that looked at many appendices --over 30,000-- to
look for the presence of the abnormal prion protein and what they found was
about 16 out of 32,000 cases were positive for variant CJD and that there
really wasn't any difference in the number of cases depending on when these
patients were born are you going to talk a little bit about that about what that
means no okay and that all codon 129 polymorphisms
were represented so this led to the estimation that about one in 2,000
citizens of UK are harboring asymptomatic infection of prion disease
so this is why when you get a give blood in this country they give you a laundry
list of questions some of which is have you resided in the UK from this time to
this time and that's because they're trying to assess the risk of your
exposure to BSE. so changing gears a little bit to chronic wasting disease
fortunately we really don't have BSE in this country but unfortunately we have a
lot of what's called wasting disease. this is the prion
disease and deer elk moose and caribou that is a little unusual and that it
tends to be fairly infectious amongst its own species so essentially the BSE
epidemic was man-made we were kind of perpetuating the infection because we
were refeeding neural tissue back to cow's and perpetuating the infection
kind of like kuru chronic wasting disease can be transmitted between its
own species through things like saliva urine and feces so much more easily
transmitted in the natural environment which means that it spreads a lot more
rapidly and this map is just the depiction of cases of chronic wasting
disease you can see it's usually out in the Colorado Wyoming area but it has
been spreading the Canada and also to some states in the East Coast and then
in the last year so we've also heard about different cases in Norway we don't
know exactly how it got to Norway although there are some theories one is
that it's a sporadic occurrence and that just other countries haven't caught it
yet the other possibility is that hunters use urine to attract other deer
and sometimes that urine can be imported into different countries so it's
possible that there's year and contaminated with CWD that was imported
into Norway and that these deer became ill that was chronic wasting disease is
obviously very important to our country because we want to avoid what happened
in the UK with BSE luckily there's been no evidence of transmission of CWD to
humans but as with the case with the iatrogenic CJD and with BSE we only
really know that if we continue surveillance so sometimes these
incubation periods can be a decade or more
so we may not know right away whether or not it's being transmitted to humans so
this is why the CDC work and the National prion disease pathology
surveillance centers work is so important because sometimes the only way
to detect abnormal or new prion diseases is by
looking at brain tissue so part of what the surveillance centre does is it looks
for atypical prion disease that may be suggested that chronic wasting diseases
being transmitted to humans but again today we don't have any evidence that
that could happen.



 For more infomation >> Here & Now Wednesday August 29 2018 - Duration: 1:03:54.
For more infomation >> Here & Now Wednesday August 29 2018 - Duration: 1:03:54. 

 For more infomation >> RHONY: Is Andy Cohen Scared Of Bethenny Frankel? (Season 10, Episode 21) | Bravo - Duration: 2:53.
For more infomation >> RHONY: Is Andy Cohen Scared Of Bethenny Frankel? (Season 10, Episode 21) | Bravo - Duration: 2:53. 



 For more infomation >> Dragon Con is more about the costumes: Here's how they also give back - Duration: 0:58.
For more infomation >> Dragon Con is more about the costumes: Here's how they also give back - Duration: 0:58.  For more infomation >> Neighbor's dog keeps barking? Here's how to solve it - Duration: 1:17.
For more infomation >> Neighbor's dog keeps barking? Here's how to solve it - Duration: 1:17.  For more infomation >> Flu Season Almost Here - Duration: 1:26.
For more infomation >> Flu Season Almost Here - Duration: 1:26.  For more infomation >> If Trump slaps auto tariffs on Canada, here's what you'll pay - Duration: 3:04.
For more infomation >> If Trump slaps auto tariffs on Canada, here's what you'll pay - Duration: 3:04. 
 For more infomation >> National Slinky Day is here and it's awesome - Duration: 2:17.
For more infomation >> National Slinky Day is here and it's awesome - Duration: 2:17. 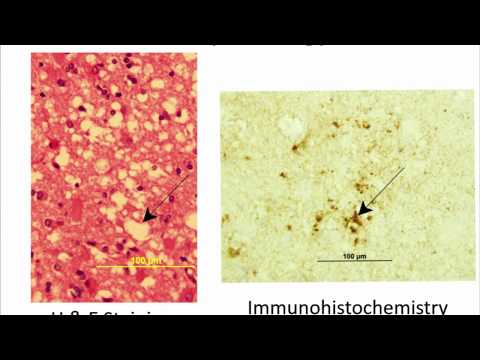
Không có nhận xét nào:
Đăng nhận xét